Return of spontaneous circulation (ROSC) is the return of a palpable pulse and substantial breathing effort after cardiac arrest.
Patients with ROSC may not regain consciousness
Signs of ROSC include
Breathing (or recognizable breathing effort, not occasional gasps)
Coughing
Movement (may not be purposeful)
Palpable pulse
Measureable blood pressure
Sudden increase (>10 mmHg) in end-tidal CO2 (EtCO2) on waveform capnography
Post Arrest Care
Ischemia may cause cardiac malfunction, which lasts for hours post resuscitation. Compromised tissue and organ function due to shock and respiratory failure may negatively impact oxygenation and perfusion.
Post resuscitation priorities include:
Maintaining adequate blood pressure and cardiac output
Restoration and maintenance of oxygenation and perfusion
Improving preload
Treating cardiac dysfunction, including arrhythmias
Maintaining Hgb levels within a normal range
Using energy-saving therapies such as mechanical ventilation and hypothermia as indicated
Evaluate and Identify
Monitor
Heart rate rhythm, BP, and pulse pressure
Urinary output
In ICU settings, measure BP via arterial line (A line), central venous pressure (CVP), central O2 levels, and cardiac output using advanced technologies
Physical Assessment
Perform frequently
Pay attention for signs of good/poor perfusion
Monitor end-organ function to evaluate perfusion
Tests
Arterial blood gas (ABG)
Hemoglobin and hematocrit
Glucose, CBC, electrolytes, liver and renal panels, calcium lactate
Oxygen saturation (O2 sat)
Troponin levels
Chest X-ray (CXR)
12-lead ECG
Echocardiogram
Intervene
Intravascular Volume
Obtain secure venous access; using at least 2 sites if possible.
Administer fluid boluses of 10-20 mL/kg isotonic solution over 5-20 minutes to restore intravascular volume. If heart failure is present, administer fluid boluses of 5-10 mL/kg isotonic solution over 10-20 minutes as needed.
Consider administration of colloids or blood products if indicated.
Blood Pressure
Treat hypotension aggressively.
Use fluids or vasoactive medications.
If hypertension occurs, evaluate cause. Causes may include medication, pain, seizures, or anxiety.
Arrhythmias
Control with medication and/or electrical therapy
Consult pediatric cardiologist
Oxygenation and Perfusion
High concentration oxygen
Titrate SpO2 to 94%-99%
Consider administration of RBCs
Consider positive pressure ventilation
Metabolic Needs
Intubate and provide mechanical ventilation if indicated
Control pain, agitation, and anxiety
Use antipyretics if fever is present
Myocardial Dysfunction
Expect dysfunction for 24 hours post arrest
Manage with medications
Correct underlying problems that add stress to the cardiovascular system
Targeted Temperature Management
Controlled trials have failed to show a benefit of targeted temperature management in comatose children after resuscitation from arrest in the hospital. Thus, routine use of targeted temperature management is not recommended. On the other hand, fever should be avoided or aggressively treated in comatose children after resuscitation.
It is reasonable for children who had arrest outside of the hospital to be treated with 5 days of normothermia (36°C to 37.5°C) or 2 days of continuous hypothermia (32°C to 34°C) followed by 3 days of normothermia.
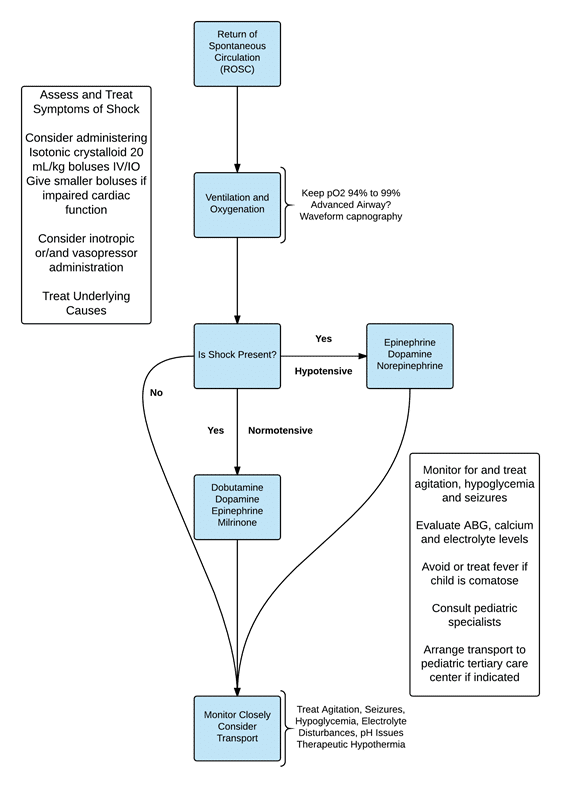
Post Resuscitation Management of Shock
Shock may occur post resuscitation due to blood loss, impaired contractility of the heart, changes in vascular resistance, or increased pulmonary vascular resistance
Perfusion may be improved by enhanced by
Increasing preload with fluid boluses
Improving contractility via the use of inotropes or inodilators. Treating poisonings, drug toxicities, hypoxia, and electrolyte imbalances improves contractility. Measures which correct acid–base imbalances, hypoglycemia, and hypocalcemia—enhance contractility
Improving afterload with vasopressors or vasodilators
Controlling heart rate. Epinephrine and antiarrhythmics may be useful indicated. Pacing and correction of hypoxia helps to normalize the heart rate
Administer fluids and vasoactive medications to enhance renal perfusion and restore acid-base balance
If fluid overload is suspected, employ diuretics such as furosemide (Lasix)
Avoid medications that are detoxified via the kidneys if urinary function is impaired
Restrict fluids in oliguric children if intravascular volume is adequate in case renal failure is present
Consider the use of sodium bicarbonate
PostResuscitation: Gastrointestinal System
Goals
Restore and maintain GI, hepatic, and pancreatic function
Minimize aspiration
Support perfusion
Prevent and relieve distention
Correct electrolyte imbalances that may contribute to ileus formation
Evaluate and Identify
Monitor gastric drainage
Perform an assessment of the abdomen
Labs include: LFTs, amylase, lipase levels, and studies to evaluate acid-base balance
Assess for signs of bowel ischemia
Imaging studies may include CT scan of the abdomen and ultrasounds of the pelvic and abdominal organs
Intervene
For gastric distention, insert an OG or NG tube. A sump tube is superior to a single lumen feeding tube
To prevent and treat ileus formation, insert OG or NG tube and connect to continuous suction; monitor and maintain a healthy balance of electrolytes
If liver failure occurs, infuse glucose; if bleeding occurs, administer blood products as needed
PostResuscitation: Hematological System
Goals
Optimization of the oxygen carrying capacity of blood
Restore and/or maintain coagulation function
Evaluate and Identify
Conduct a physical assessment to monitor for signs of internal or external bleeding
Evaluate skin and mucous membranes for pallor, petechiae, or bruising
Laboratory studies include CBC, Hgb, Hct, PT, PTT, D-dimer, INR
Intervene
If hemorrhagic shock occurs, administer isotonic crystalloid and PRBCs
Use platelets to correct thrombocytopenia
Seek expert assistance for massive hemorrhages
Administer FFP if the child is bleeding, at risk for bleeding,or has abnormal clotting study results
If the PT is elevated, administer Vitamin K
Transport of the Critically Ill Child
Planning and Communication
Assessment, monitoring, treatment, stabilization, communication, and documentation skills are needed before, during, and after transport. These aspects are important whether a patient is being transported between facilities or between units.
A transport plan requires coordination between personnel from the sending and receiving facilities as well as with the transport team.
Excellent communication with the child’s family is critical
Regulationsand Preparation
The federal Emergency Medical Treatment and Active Labor Act, (EMTALA) regulates transport between facilities.
Advance preparation for transport of patients includes identification of tertiary care facilities and transport agencies, maintain supplies, and transport protocols.
If an infectious illness is suspected, cultures must be obtained and antibiotics administered. Personnel from the sending facility must notify the transport team and receiving facility workers to ensure that proper precautions are made. Use universal precautions for all patients. Employ additional precautions if a communicable disease is suspected.
Obtain written consent from the child’s parents/guardians prior to transport.
Consider advanced airway placement prior to transport if the child does not have one. Confirm placement.
Stabilize the child.
Ensure that all equipment is securely attached.
Provide analgesia and sedation prior to transport if indicated.
Copy medical records.
Prepare medication, blood products, and infusions needed for transport.
Optimization of the oxygen carrying capacity of blood.
Restore and/or maintain coagulation function.
The referring physician is responsible for notifying the receiving facility if a child’s condition changes after the initial report to the receiving facility was conducted.
Reports, documentation, transport
Date, time, vital statistics, medical history, current problem, medications, fluids, equipment in use, presence of infectious disease, family contact information, labs and imaging results, assessment, information about care provided to stabilize child, reason for transfer, name of receiving physician and facility.
Document names of people who report was provided to and any other pertinent information.
Follow facility guidelines and federal regulations regarding providing and obtaining follow-up information.
The majority of transports occur via ground ambulance. Helicopters are used for longer distance transports. Children who have a surgical emergency may benefit from helicopter transport. Fixed wing airplanes are used to transport children from remote locations and for long distance trips.
Pediatric Critical Care Transport Team
Volunteer or professional EMS personnel, pediatric transport experts, personnel from the referring facility, and critical care transport experts.
Engage a pediatric transport team if the child:
Requires intensive care services from the receiving facility
Has a significant risk of cardiopulmonary or neurologic deterioration during transport
Is stable, but has just survived a life-threatening event, such as cardiac arrest, SIDS, status epilepticus, or severe shock
Has experienced a life-threatening event that has a high probability of recurrence
It is often preferable to wait for the arrival of a specialized pediatric transport team even if it delays transport.
If a child needs an immediate surgical intervention, do not wait for a specialized team.
Broad criteria are used to determine whether a special pediatric transport team is utilized.