NATIONALLY ACCEPTED
Accepted in all 50 states instantly
ILCOR & ECC STANDARDS
Our Courses are as per guidelines
ONLINE ACCESS 24/7
All of our services are 100% online

Key Definitions
ARDS: Acute respiratory distress syndrome
Arterial O2 Content: Total oxygen in the blood. It is a combination of bound O2 (attached to hemoglobin) with non-bound O2 in the blood
CPAP: Continuous positive airway pressure
Hemoglobin, Hgb: Molecule that carries oxygen in red blood cells
Oxygen saturation, O2sat: The amount of oxygen that is bound to hemoglobin.
PaCO2: Arterial tension of carbon dioxide
PaO2: Arterial tension of oxygen
PEEP: Positive end-expiratory pressure
PO2: Atmospheric pressure of oxygen
SpO2: Oxygen saturation level monitored by pulse oximetry
V/Q Mismatch: V is ventilation; Q is blood flow to lung (perfusion). Simply put, blood is flowing to the lungs, but the blood is not being oxygenated by the lung tissue.
A person with absent or ineffective breathing and a pulse should be treated with rescue breathing, not chest compressions. If the person in respiratory arrest loses their pulse during resuscitation, he or she should be treated as cardiac arrest.

Identify Early, Intervene Early
Untreated respiratory distress will progress to respiratory failure
Untreated respiratory failure will progress to respiratory arrest
Unresponsive, unconscious, and a lack of effective breathing à Start rescue breathing!
| Qualities | Respiratory/ Cardiac | Breath Sounds | Causes | Additional Information |
| Upper Airway Obstruction | Tachypnea Accessory muscle use Poor chest rise | Hoarse, cry, barking, stridor Diminished air entry | Foreign body, swelling of upper airway, mass in airway, secretions, congenital, intubation | Signs most noticeable during inspiration |
| Lower Airway Obstruction | Tachypnea Retractions, nasal flaring, prolonged exhalation | Wheeze, cough | Asthma, bronchiolitis | Signs most noticeable during exhalation |
| Lung Disease | Tachypnea, tachycardia, increased work of breathing | Grunting, crackles, diminished breath sounds | Pneumonia, pulmonary edema, allergy, trauma, pulmonary infiltrates | Signs of hypoxemia |
| Disordered Breathing Control | Signs of inadequateor variable respiratory effort, irregular respiratory rate/ bradypnea/tachypnea | May be none due to central apnea without respiratory effort | CNS illness and trauma | Decreased level of consciousness Shallow breathing |
Techniques used to treat upper airway obstruction
| Mild | Moderate | Severe | Impending Respiratory failure | |
| Symptoms | Occasional barking cough, minimal or no stridor at rest, minimal or no retractions | Frequent barking cough and retractions while resting, little or no agitation, auscultation reveals good air movement of peripheral lung fields | Frequent barking, pronounced inspiratory and occasional expiratory stridor, marked retractions, agitation, poor air movement within lungs | Barking cough which may weaken, hypoxemia, hypercarbia, retractions which may weaken, lethargy, decreased level of consciousness, pallor, cyanosis, poor air movement within lungs |
| Interventions | Dexamethasone | Dexamethasone Humidified O2 Nebulized epinephrine Monitor for a minimum of 2 hours after epinephrine administered Consider Heliox (helium plusO2) | Dexamethasone Humidified O2 Nebulized epinephrine Monitor for a minimum of 2 hours after epinephrine administered Consider Heliox (helium plus O2) | Dexamethasone High concentration O2 with non-rebreather mask Bag valve mask if O2 sat persists <90% or if level of consciousness decreases Insert ET tube (use ½ size smaller than usually indicated for child’s age; should only be performed by trainedteam member) Prepare for surgical airway |
| Symptoms | Mild | Moderate/ Severe | Impending Respiratory Failure |
| Breathlessness | Talks in sentences | Talking in phases or words Sits hunched over Not eating (infants) | Unable to talk speak or eat |
| Wheeze | Often only on exhalation | Loud | Absent |
| Accessory muscle use | No | Usually | Weak |
| Retractions | No | Usually | Paradoxical movements |
| Respiratory rates | Increased respiratory rate | Elevated respiratory rate | Respirations may be absent |
| Heart rates | Elevated or normal | Markedly elevated | Bradycardia |
| Pulsus paradoxus | No or <10 mmHg | Often present >10-25mmHg | Absent |
| PaO2 on air | Normal | >60% moderate;<60% severe | |
| PaCO2 on air | <45 mmHg | <45% moderate; >45% severe | |
| SaO2 % | >95% | 91%-95% moderate; <90% severe | |
| Alertness | Agitation | Agitation | Decreased |
| Mild | Moderate/ Severe | Impending Respiratory Failure | |
| Oxygen | Humidified high concentration oxygen via nasal cannula or mask Titrate to keep SpO2 sat >94% | Humidified high concentration oxygen via mask Non-rebreather mask may be needed Titrate to keep SpO2 sat >94% | Humidified high concentration oxygen via non-rebreather mask |
| Medications | Albuterol via MDI or nebulizer Oral corticosteroids | Albuterol via nebulizer Oral or IV corticosteroids Consider magnesium sulfate to be given over 15-20 minutes | Albuterol via continuous nebulizer IV corticosteroid Terbutaline IV or SQorEpinephrine SQ or IV |
| Additional Intervention | Monitor pulse and BP while administering MgSO4 | Monitor for signs of toxicity if using Terbutaline Consider BPAP ET tube insertion (consider cuffed ET tube |
| Condition | Characteristics/ Etiology | Ventilation | Medications | Diagnostic Tests | Additional Information |
| Infectious pneumonia | Caused by microorganisms Often community acquired | CPAP ET intubation and mechanical ventilation if severe | Antibiotics Nebulizer | Chest x-ray/CT, ABGs, CBC, blood cultures | Reduce fever with medication and cooling techniques |
| Chemical pneumonitis | Results from dust, fumes, toxic gases, smoke, and particles | CPAP Non-invasive ventilation, Intubation, mechanical ventilation | Nebulized bronchodilators | May require rapid transport to a specialized facility, as advanced technology may be needed | |
| Aspiration pneumonitis | Chemical pneumonitis due to inflammation caused by gastric or oral secretions | CPAP Non-invasive ventilation, Intubation, mechanical ventilation | Antibiotics if lung infiltrates present on x-ray | Chest x-ray/CT | |
| Cardiogenic pulmonary edema | High pressure in pulmonary vessels causes fluid to accumulate in the lung tissues. Left ventricular cardiac disease or abnormalities, inflammatory processes, drugs, and hypoxia cause edema | Non-invasive ventilation or intubation with mechanical ventilation PEEP Intubation and mechanical ventilation indicated if hypoxia is persistent, respiratory failure imminent, or hemodynamically unstable | Diuretics Inotropic infusions Afterload reducing drugs | Obtain specialist consultation Normalize temperature PEEP usually at 6-10 cm H2O. Too much PEEP can be harmful | |
| Non cardiogenic pulmonary edema (ARDS) | Usually secondary to a systemic or respiratory illness Acute onset, bilateral lung infiltrates, no cardiac cause | Non-invasive ventilation or intubation with mechanical ventilation PEEP Intubation and mechanical ventilation indicated if hypoxia is persistent, or worsening lung condition | Monitor vital signs pulse oximetry, end tidal CO2 levels, ABGs , central venous blood gas, CBC | Early recognition and TX of shock, bacteremia, and respiratory failure may prevent ARDS Increase PEEP until oxygenation adequate. Correction of hypoxia is most important goal even if hypercarbia |
| Condition | Characteristics/ Etiology | Ventilation | Medications | Diagnostic Tests | Additional Information |
| Respiratory failure/distress with increased intracranial pressure | Brain infections, TBI, brain tumor, subarachnoid bleed, hydrocephalus | Use jaw thrust if needed to open airway if trauma present May need transient hyperventilation | May need LR or NS infusion at rate of 20 mL/kg if not perfusing well | Lumbar puncture | Irregular respiratory pattern may indicate increasing ICP. Cushing’s triad =bradycardia, irregular respirations or apnea, and increased mean arterial pressure may indicate impending brain herniation. Decerebrate or decorticate posturing, HTN, and abnormal pupils indicative of herniation. Neurosurgical consult needed |
| Respiratory distress/failure secondary to drug overdose or poisoning | Depression, weakness or cessation of respiratory drive,altered rate of respirations;other respiratory impairments may occur simultaneously | Suction airway | Antidote | ABGs , ECG, chest x-ray, electrolytes, glucose, serum osmolality, drug screen | Notify Poison Control if poisoning suspected (1-800-222-1222) |
| Respiratory distress/failure secondary to neuromuscular disease | Neuromuscular diseases Ineffective cough, inability to clear secretions, atelectasis, pneumonia may occur | May need long-term non-invasive ventilation | Electromyography, nerve conduction studies | Some commonly used emergency drugs may cause life threatening complications for children with neuromuscular diseases, including succinylcholine and aminoglycosides |
Simple (Non-advanced) Airways
The simplest way to open the airway is the head tilt-chin lift maneuver:
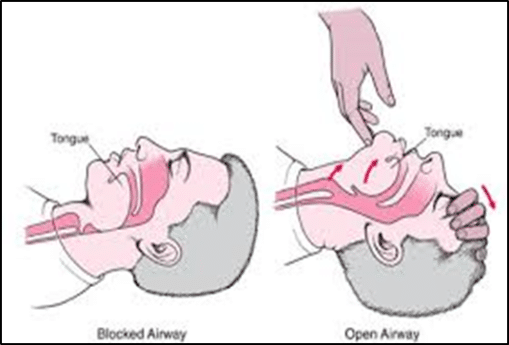
If you suspect an injury to the neck, use the jaw thrust technique instead:

Mouth-to-mask resuscitation is appropriate


An oropharyngeal airway is:
Proper Sizing:
Should span from side of jaw to corner of mouth
Too large and it will occlude the larynx, and too small will not be effective


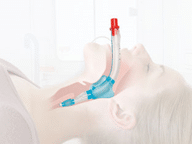
A nasopharyngeal airway is:

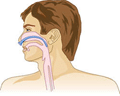
Proper Sizing:
Should span from tip of nose to earlobe
Too large and it will occlude the larynx, and too small will not be effective

Advanced airways require advanced training to insert that is beyond the scope of ACLS. However, ACLS providers may use them once they have been placed.Advanced airways include:
Laryngeal mask airway

Laryngeal tube
Esophageal-tracheal tube (Combitube)

Endotrachealtube



