In cardiac arrest, ventricular fibrillation and pulseless ventricular tachycardia are considered “shockable” rhythms. This means that an unsynchronized defibrillation or shock energy from an AED or manual defibrillator can be used to restore a normal cardiac electrical rhythm.
Ventricular tachycardia in a person with a pulse is not cardiac arrest; however, a cardiac rhythm of ventricular tachycardia may progress to cardiac arrest within seconds, and so must be evaluated and treated emergently.
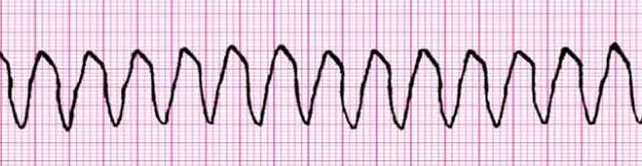
Ventricular Tachycardia
Wide complex tachycardia,QRS >120 msec
Monomorphic
Regular
Ventricular Fibrillation (VFib)
Wide complex
Polymorphic: Can be coarse or fine
Fine Vfib is important to differentiate because it can appear like asystole on monitor
Makes the difference between shockable and unshockable rhythm
Torsades de Pointes
Torsades de Pointes (“twisting of the points”) is an unusual form of polymorphic ventricular tachycardia
Patients will usually have a palpable pulse and be conscious
If there IS a pulse, it is NOT cardiac arrest – Treat with magnesium sulfate
If there is NO pulse, it IS cardiac arrest – Treat as pulseles V-Tach/V-Fib
Defibrillation – Manual Defibrillator and AED Use
Out of hospital cardiac arrest is usually treated with an AED
In-hospital cardiac arrest is usually treated with a manual defibrillator
AED Use
Keep giving chest compressions until AED is ready to analyze (i.e., pads are in place)
Place pads correctly and ensure that they are the appropriate size for the patient
Remove chest hair and sweat, as these can negatively affect conduction of electricity
ALWAYS CLEAR THE PATIENT BEFORE DELIVERING SHOCKS
Perform visual check to ensure no one is touching the patient before delivering shock
Announce “Clear” before shocking
An AED will automatically provide the right “dose” of electrical energy
As soon as a shock is delivered, IMMEDIATELY resume CPR and give appropriate medications
Manual Defibrillator Use
Keep giving chest compressions until defibrillatoris ready to analyze (i.e., pads are in place)
Place pads correctly and ensure that they are the appropriate size for the patient
Some manual defibrillators use paddles instead of pads
Remove chest hair and sweat, as these can negatively affect conduction of electricity
ALWAYS CLEAR THE PATIENT BEFORE DELIVERING SHOCKS
Perform visual check to ensure no one is touching the patient before delivering shock
Announce “Clear” before shocking
Defibrillator can be monophasic or biphasic
Monophasic: Defibrillate at 360 J
Biphasic
Use the manufacturer’s recommended dose for the defibrillator (120-00 J)
If you do not know the recommended dose, use maximum biphasic dose
If unsure of the type of defibrillator, defibrillate at 360 J
As soon as a shock is delivered, IMMEDIATELY resume CPR and give appropriate medications
Medications Used in pulseless VTach/VFib
Epinephrine (1 mg IV) can be given after the second unsuccessful shock
The term “unsuccessful” means that there has NOT been return of spontaneous circulation (ROSC)
Amiodarone can be given after third unsuccessful shock
Give 300 mg IV first dose
May give an additional dose of 150 mg IV
Lidocaine can be given only if amiodarone is not available
Give 1 to 1.5 mg/kg IV.
If the first dose is not effective, give half doses of lidocaine every 5-10 minutes
Maximum: 3 mg/kg IV
Magnesium sulfate is used to treat Torsades de Pointes
Loading dose: 1-2 g IV/IO diluted in D5W or NS, infuse over 5-20 minutes